


By Erin Heilman May 13, 2022 Regulatory Updates: Ambulatory,Regulatory Updates: Hospital
CMS’s Promoting Interoperability requirements vary depending on if you’re a hospital or ambulatory practice. Find out which requirements matter to you—and which ones you can happily ignore.
How to Unpack Your Promoting Interoperability Requirements
If you’re having trouble deciphering which CMS Promoting Interoperability requirements apply to you, you’re not alone. According to our Medisolv Clinical Quality Advisors, Promoting Interoperability is one of the most frequent sources of questions, confusion, and pencil-snapping frustration among the quality program managers that we talk to every day.
So, we here at Medisolv think it’s time to unpack Promoting Interoperability and help you sort out which requirements matter to you—and which ones you can happily ignore.
The first rule of PI Club: How you report depends on who you are
CMS offers two forks in the road for how you can report Performance Interoperability: (1) the Medicare Promoting Interoperability Program or (2) the MIPS Program’s Promoting Interoperability Category. Which fork you take depends on what type of reporting entity you are:

- If you report as a hospital or critical access hospital, you are responsible for participating in the Medicare Promoting Interoperability Program.
- If you report as a non-hospital-based clinician or physician group, you are responsible for submitting data through the Promoting Interoperability Category within your MIPS program.
If you’re part of an APM, you’ll still need to submit your Promoting Interoperability data at the individual or group level through traditional MIPS. APMs themselves do have separate requirements around certified health IT, and those requirements vary from APM to APM. While we won’t be taking a deep dive on that topic in this post, ONC has identified some commonalities around APMs and certified health IT if you’re interested in learning more.
Do these two Promoting Interoperability programs have any requirements in common?
Yes, they actually do! Regardless of whether you’re a hospital reporting through the Medicare Promoting Interoperability Program or an ambulatory practice reporting through MIPS, there are some basic requirements that both programs share:
- A 90-day EHR reporting period (hospitals) or performance period (clinicians)
- Use of either the 2015 Edition certification criteria, the 2015 Edition Cures Update Criteria, or a combination of the two for the entirety of the reporting/performance period. Medisolv is already using certified to the Cures Update which is required next year.
- 4 objectives (i.e., categories) that you must report: the Public Health & Clinical Data Exchange objective; the Electronic Prescribing objective; the Provider to Patient Exchange objective ; and the Health Information Exchange objective.
- A ‘yes’ submission to the ‘action to limit or restrict the compatibility or interoperability of CEHRT’ attestation.
- A ‘yes’ submission to the Security Risk Analysis measure, an attestation that you’ve completed your annual security risk assessment.
New this year, both programs will also offer a single Health Information Exchange (HIE) Bi-Directional Exchange measure that you’ll have the option to submit in place of the two traditional HIE objective measures. Learn more >>
How is Promoting Interoperability different for hospitals?
Once you’ve checked off the requirements listed above, reporting as a hospital to the Medicare Promoting Interoperability Program is quite different than reporting as an ambulatory practice through MIPS. Here are the key distinctions that you need to remember:
Your Public Health and Clinical Data Exchange objective has 4 requirements
While most of the objectives in the Medicare Promoting Interoperability Program are only comprised of 1 required measure, the Public Health and Clinical Data Exchange objective has 4 measures that you must report:
- Syndromic Surveillance Reporting
- Immunization Registry Reporting
- Electronic Case Reporting
- Electronic Reportable Laboratory Results
Note that this is different than the MIPS program for clinicians; they only have to report on 2 required measures under this objective, Immunization Registry and Electronic Case Reporting.
You have to achieve a minimum score of 60
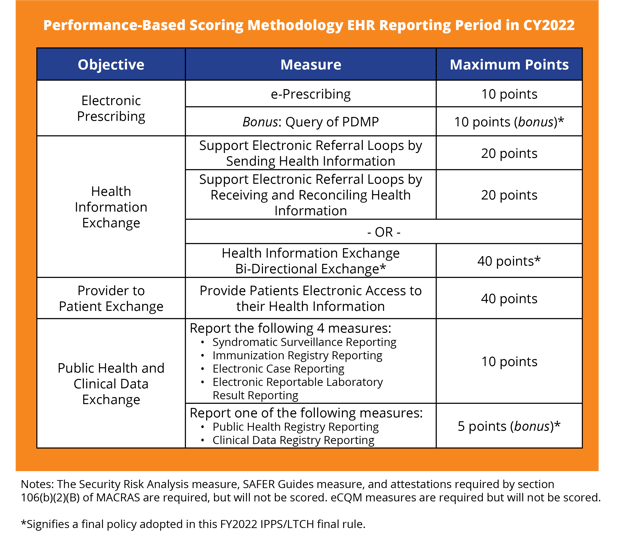
For 2022, you must score 60 points minimum out of a total of 100 points, or 115 points if you include the currently available bonuses. This year, bonuses can be earned by reporting the Prescription Drug Monitoring Program optional measure in the Electronic Prescribing objective (10 points), and for submitting one of two optional measures in the Public Health and Clinical Data Exchange objective: Public Health Registry Reporting or Clinical Data Registry Reporting (5 points).
You have to attest to using (or not using) all 9 SAFER Guides
The Safety Assurance Factors for EHR Resilience (SAFER) Guides are a new requirement for 2022 designed to help you optimize the safety and safe use of your EHRs. While the MIPS program only requires clinicians to complete an annual assessment of one SAFER Guide (the High Priority Practices Guide) the Medicare Promoting Interoperability Program requires your hospital to complete an assessment of all 9 SAFER Guides:
- High Priority Practices
- Organizational Responsibilities
- Contingency Planning
- System Configuration
- System Interfaces
- Patient Identification
- Computerized Provider Order Entry with Decision Support
- Test Results Reporting and Follow-up
- Clinician Communication
The good news is that, at this point, CMS is only tracking if hospitals are using the Guides. So, you can attest ‘Yes’ or ‘No’ without getting a penalty. If you’re new to the concept of SAFER Guides, we’ve created a detailed primer to help you understand each Guide and how to use them.
More key differences for hospitals:
- Along with all your other data, you must submit 4 eCQMs covering 3 quarters of data. However, if you submit your eCQMs through an IQR program, then you do not need to submit them again.
- While clinicians participating in the MIPS program have multiple ways to submit data, hospitals are only able to submit through the CMS Hospital Quality Reporting System (aka the QualityNet Secure Portal).
- If you need to apply for a hardship exception, applications are available AFTER the data submission period has ended.
How is Promoting Interoperability different for clinicians?
While hospitals have to manage their IQR and Promoting Interoperability efforts as two entirely separate programs, clinicians have it bit easier, at least on paper. That’s because Promoting Interoperability is just 1 performance category out of the 4 total that make up the overall MIPS program.
In fact, when it comes to Promoting Interoperability for clinicians, ease of use seems to be the key difference across the board:
- Clinicians have 3 options for submitting data versus the hospitals’ one: (1) attesting through qpp.cms.gov, (2) uploading your data through qpp.cms.gov, or (3) using a third party like Medisolv to submit your data.
- While hospitals have to report on 4 required measures under the Public Health and Clinical Data Exchange objective, clinicians only have to report on 2: Immunization Registry Reporting and Electronic Case Reporting.
- Clinicians only have to attest to 1 SAFER Guide (the High Priority Practices Guide), while hospitals have to attest to all 9.
- Hardship exception applications are available prior to your data submission period (hospitals have to wait until after).
But don’t snooze: Promoting Interoperability is still 25% of your score
Even if you ace your Promoting Interoperability category, that will only net you 25 points towards achieving the MIPS 75-point penalty avoidance threshold for 2022. Because the threshold is the highest it’s ever been, every single point is crucial this year. Fortunately, like hospitals, you do have the opportunity to earn up to 5 bonus points for reporting at least one extra Public Health Registry (Public Health, Clinical Data, or Syndromic Surveillance) and another 10 bonus points for submitting the Query of Prescription Drug Monitoring Program optional measure.
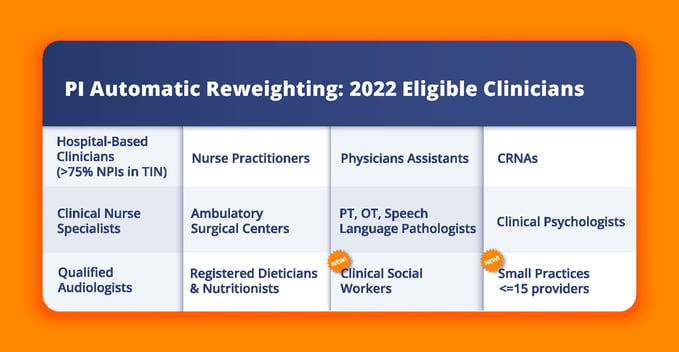
Determine if you’re eligible for automatic reweighting
Keep in mind that CMS automatically reweights the Promoting Interoperability category for a selection of Eligible Clinicians. If you qualify for automatic reweighting, you do NOT have to report Promoting Interoperability and you no longer need to apply for a hardship exception in this category. In fact, if you do submit Promoting Interoperability data, it will override your exception and count toward your final score. So just sit back, relax, and let the automatic reweighting do its job.
Don’t Worry: You’ve Got This (And Us)
Once you understand which program and requirements applies to you—and which ones you can ignore—navigating Promoting Interoperability becomes easier. CMS has even created a cheat sheet to help you quickly and visually identify the differences that matter to you.
And don’t forget, Medisolv’s Clinical Quality Advisors are always on hand to help you translate CMS-speak into real, manageable steps you can take to make sure you’re not only meeting your Promoting Interoperability requirements but also achieving the requirements’ ultimate goal: better patient care through the power of more accessible data.
Contact us now to schedule a time to chat, or check out our other resource guides for more info:
- Understanding SAFER Guides & 2022 PI Requirements (For Hospitals)
- 2022 IQR and PI Program Changes: A Summary From the IPPS Final Rule
- The 10 Biggest Takeaways for MIPS Success in 2022
- What is Health Information Bi-Directional Exchange?
Medisolv Can HelpAlong with award-winning software, each client receives a dedicated Clinical Quality Advisor that helps you with your technical and clinical needs. We consistently hear from our clients that the biggest differentiator between Medisolv and other vendors is the level of one-of-one support. Especially if you use an EHR vendor right now, you’ll notice a huge difference.
|


Add a comment