
.png?width=900&height=600&name=BlogImage_2025%20APP%20Reporting%20Requirements%20for%20ACOs%20(2).png)
The Quality Payment Program (QPP) has allowed large organizations to use the CMS Web Interface reporting method to complete MIPS requirements since the program launched in 2017. This gave these organizations the option to report a sampling of 248 patients (selected by Medicare Part B claims) across all their practices. CMS completely sunset the CMS Web Interface reporting option in 2025.
In 2025, all MSSP ACOs must report either eCQMs, CQMs, or Medicare CQMs across all of their practices for 365 days of the year.
Figuring out data aggregation, de-duplication, and comprehensive performance review is the key to your 2025 reporting success. Below is a summary of your 2025 APP requirements.
2025 APP Reporting Requirements
There are three reporting frameworks available in the Quality Payment Program, but MSSP ACOs can only submit to one, the APM Performance Pathway (APP) reporting framework.
Also read: A comparison of the 2025 requirements for all three reporting frameworks.
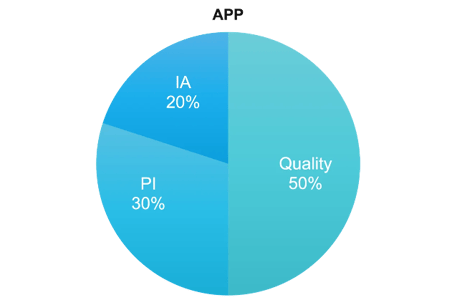
APP Framework Category Weights
For the APP framework, there are three categories, Quality, Promoting Interoperability, and Improvement Activities. Cost is weighted at 0%.
Defining QPP Collection Types
Collection types are the way you report the data to CMS. You can think of them like measures. There are five collection types in 2025.
- eCQMs
- MIPS CQMs
- Medicare CQMs
- Medicare Part B Claims measures
- CAHPS for MIPS survey
Quality Category Requirements
Category weight: 50% of total score
Performance Period: 365 days
Requirements:
- Submit all measures in the APP Plus Measure Set
- Meet data completeness requirement
- Meet case minimum criteria
- Can use combination of collection types
- One administrative claims measures is calculated and scored automatically
Measure list:
- Quality Measures (eCQMs/CQMs/Medicare CQMs)
- Quality ID: 001 Diabetes: Hemoglobin A1c (HbA1c) Poor Control
- Quality ID: 134 Preventive Care and Screening
- Quality ID: 236 Controlling High Blood Pressure
- Quality ID: 112 Breast Cancer Screening
- Claims Measures
- Hospital-Wide, 30-day, All-Cause Unplanned Readmission (HWR) Rate for MIPS Eligible Clinician Groups
- CAHPS for MIPS Survey measure
Other Considerations
- CMS Web Interface Measures are not available to submit in 2025.
- Each measure must meet case minimum requirements. Most measures must have a submission of at least 20 cases.
- You must meet the 75% data completeness threshold. See the full explanation at the bottom of this article.
- Beginning in the CY 2025 performance period, ACOs are eligible to receive the complex organization adjustment when reporting eCQMs. One measure achievement point is added for each submitted eCQM.
Promoting Interoperability (PI) Category Requirements
Category weight: 30% of total score
Performance Period: 180 days
Requirements:
- Submit the required measures (measure list below)
- Attest to these two measures: Actions to Limit or Restrict the Compatibility of CEHRT & ONC Direct Review
- Have CEHRT functionality that meets ONC’s certification criteria in 45 CFR 170.315 in place by the first day of your MIPS Promoting Interoperability performance period
- Have your EHR certified by ONC to the certification criteria in 45 CFR 170.315 by the last day of your performance period
- Provide your EHR’s CMS Identification code from the Certified Health IT Product List (CHPL)
- Conduct or review a Security Risk Analysis on your CEHRT functionality on an annual basis
- Attest to conducting an annual assessment of the Safety Assurance Factors for EHR Resilience Guides (SAFER Guides)
OPTIONAL: Attest to ONC-Authorized Certification Bodies (ACB) Surveillance Attestation
MEASURE LIST:
Promoting Interoperability Measures
| Objective | Measure | Maximum Pts | Required/Optional |
| Electronic Prescribing |
E-Prescribing | 10 | Required |
| Query PDMP | 10 | Required | |
| Health Information Exchange |
Option 1: Sending Health Information Receiving and Reconciling Health Information |
15 15 |
Required to choose 1 of 3 options |
| Option 2: HIE Bi-Directional Exchange | 30 | ||
| Option 3: Enable Exchange Under TEFCA | 30 | ||
| Provider to Patient Exchange | Provide Patients Electronic Access to Health Information |
25 |
Required |
| Public Health and Clinical Data Exchange | Electronic Case Reporting | 25 | Electronic Case Reporting and Immunization Registry Required |
| Immunization Registry | |||
| Public Health Registry | 5 Bonus Points for 1 | Optional |
|
| Syndromic Surveillance | |||
| Clinical Data Registry |
Other Considerations
No practices are permitted to remain on paper. The only exception to this is if your ACO has a practice in which all eligible clinicians qualify for reweighting as a small practice or all clinicians aren't eligible to report. In that event, you simply wouldn’t need to report PI for those participants since their PI score is reweighted.
Public Health and Clinical Data Exchange Objective has two Active Engagement options that must be completed for each associated measure:
- Option 1: Pre-production and Validation
- Option 2: Validated Data Production
Clinicians are required to report level of engagement for EACH measure and must transition from option 1 to option 2 after one year.
An ACO can submit Promoting Interoperability for the individual clinicians and groups they cover. They can also tell their eligible clinicians to submit their own PI data at the individual or group level. (CMS will aggregate the data for the ACO)
Reweighting
CMS is discontinuing automatic re-weighting for the following clinician types:
- Clinical social workers
CMS will continue to automatically re-weight:
- Small practices (this is the only special status that can be applied to ACOs)
Improvement Activities (IA) Category Requirements
Category weight: 20% of total score
Requirements:
All ACOs will be automatically assigned a score of 100%, which is applied to all Eligible Clinicians reporting through their ACO.
2025 Bonus Points
Improvement Bonus: Up To 10 Points
Clinicians will be rewarded if they demonstrate improvement over their 2024 Quality score (pending there is enough data for comparison). Clinicians may earn up to 10 additional percentage points based on their improvement.
Complex Organization Adjustment: 1 Point for Each eCQM Submitted
This is available for ACOs reporting eCQMs. CMS will add one measure achievement point for each submitted eCQM. The adjustment may not exceed 10% of the total available measure achievement points in the quality category.
Small Practice Bonus: 6 Points
Clinicians in small practices who submit at least one Quality measure, either individually or as a group, will receive an additional six points in the quality performance category score. This applies to ACOs with the small practice designation as well. However, this bonus is not applicable to clinicians or groups scored under facility-based scoring.
Achieving Shared Savings in 2025
In 2025, for an MSSP ACO to get the maximum shared savings for your ACO you must:
- Meet or exceed the minimum savings rate (MSR) as set by the ACO when establishing the MSSP model and track in which you choose to participate
AND - Report ALL measures in the APP Plus measure set and distribute the CAHPS for MIPS Survey
AND - Achieve the Quality Performance Standard
The Quality Performance Standard is met if you achieve a health-equity adjusted score of ≥76.70 for the Quality category.
There are two ways that make it easier to meet the Quality Performance Standard.
- If you submit eCQMs or MIPS CQMs you can score lower and still meet the Quality Performance Standard. (Not applicable to Medicare CQMs)
- Report all measures as eCQMs and/or CQMs
- Achieve a score ≥ 10th percentile on 1 outcome measure
- Achieve a score ≥ 40th percentile on at least 1 of the remaining measures
- Or if ≥ 15% of your assigned beneficiaries are enrolled in the Medicare Part D low-income subsidy (LIS) or dually eligible for Medicare and Medicaid, CMS will positively adjust your score.
-
- Your ACO will receive a Health Equity Benchmark Adjustment (HEBA) to your quality score based on the proportion of underserved beneficiaries you serve.
- If either your Positive Regional Adjustment or Prior Savings Adjustment is higher than the HEBA, CMS will take the highest of these three values to positively adjust your score.
How do I know what performance to aim for?
CMS uses historical benchmarks to determine what performance score equals which decile. The decile is the points you get for that measure. So, to achieve the 40th percentile on a measure, you must achieve the performance score at or above decile 4. You can find these benchmarks in the QPP Resource Library.
For Medicare CQMs only, CMS established flat benchmarks.
Flat Benchmarks for Non-Inverse Medicare CQMs:
| Decile | Performance Rate Range |
| 1 | <10.00 |
| 2 | 10.00 - 19.99 |
| 3 | 20.00 – 29.99 |
| 4 | 30.00 – 39.99 |
| 5 | 40.00 – 49.99 |
| 6 | 50.00 – 59.99 |
| 7 | 60.00 – 69.99 |
| 8 | 70.00 – 79.99 |
| 9 | 80.00 – 89.99 |
| 10 | ≥90.00 |
Other Considerations
CMS has implemented a sliding scale to give ACOs some percentage of the Shared Savings (not max) if they don’t meet the quality performance standards but do achieve a quality performance score equivalent to or higher than the 10th percentile of the performance benchmark on at least one of the four outcome measures. The ACO’s health equity adjusted quality performance score will be multiplied by the maximum sharing rate for the ACO’s track to determine its final shared savings rate.
For ACOs in their first performance year of their first agreement period, they can achieve the Quality Performance Standard by meeting the MIPS data completeness requirement on the 4 eCQMs/MIPS CQMs/Medicare CQMs in the APP Plus quality measure set, receiving a MIPS Quality performance category score, and administering the CAHPS for MIPS Survey.
40th Percentile MIPS Quality Performance Category Scores Used in the Calculation of the 2025 Historical MIPS Quality Performance Category Score
|
Performance Year |
40th Percentile of the MIPS Quality Performance Category Score |
|
2021 |
77.83 |
|
2022 |
77.73 |
|
2023 |
77.54 |
|
2025 |
76.70 |
Note: Performance Years 2021 through 2023 40th percentile scores are based on performance period data.
Important Dates
January 1, 2025
The start date to track 365 days of Quality category measures.
July 4, 2025
The last day to start measures and have all practices on CEHRT for the Promoting Interoperability (PI) category to meet the minimum of 180 continuous days.
December 1, 2025
Last day of the performance period.
March 31, 2026
The last day to submit all of your performance data.
Data Completeness Requirements
There has been SO MUCH discussion on this topic. CMS attempted to make it clearer by releasing a guide to Data Completeness that further validates the 100% of eligible patients. They make it very clear that no one can be excluded from the Denominator population.
An ACO must submit their entire “universe” of patients. None of your practices can be excluded based on populations. The data completeness threshold really would only be applicable in a MIPS CQM situation, and even in that situation you still must have the entire universe of practices/patients and only achieve 70% completeness on the denominator patients.
Take a look at pages six and eight of the APP guidance document here.
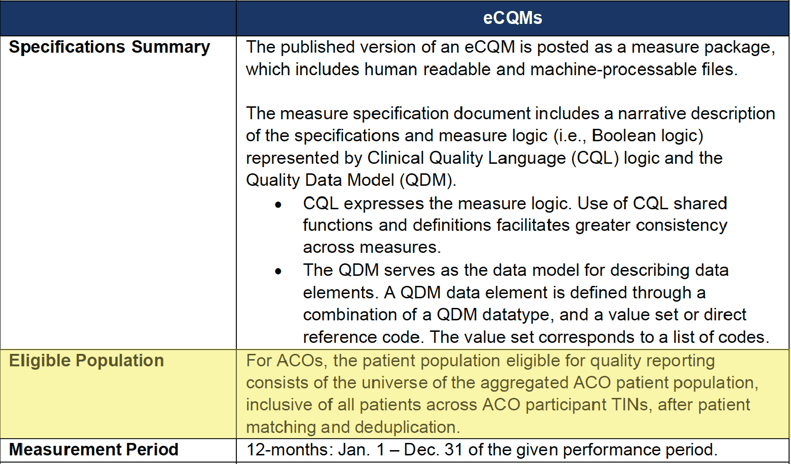
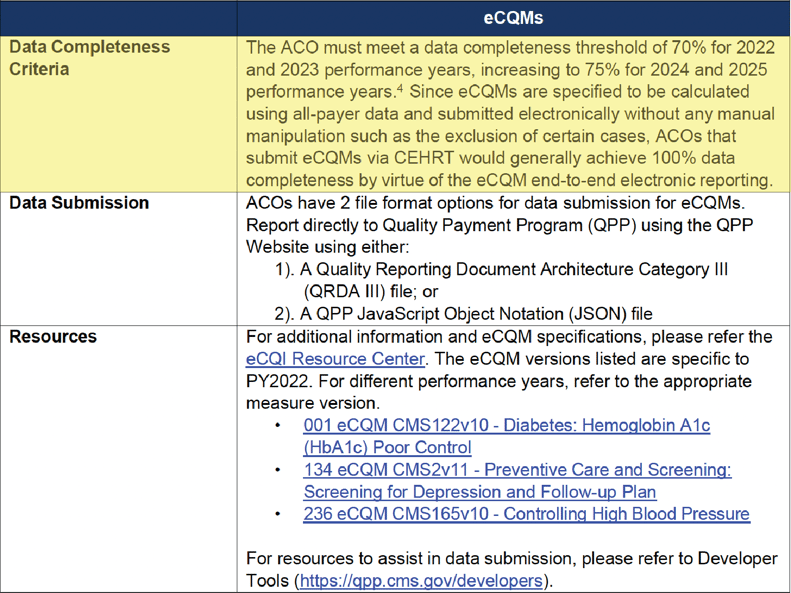
eCQM Data Completeness Criteria Summary
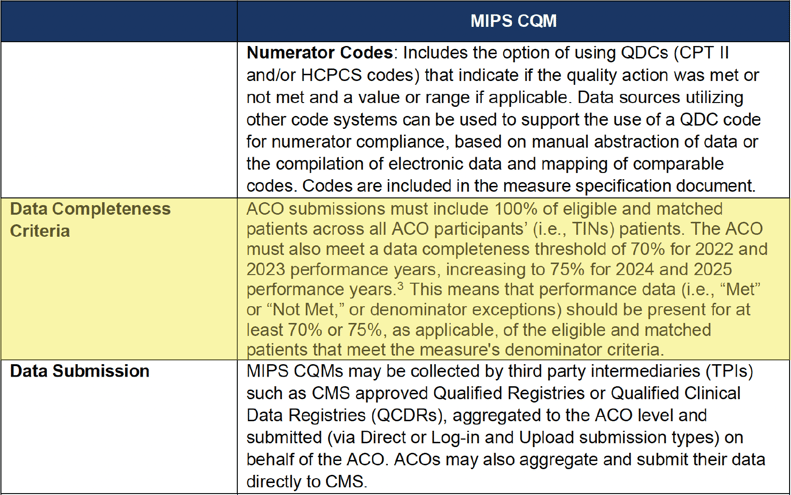
MIPS CQM Data Completeness Criteria Summary
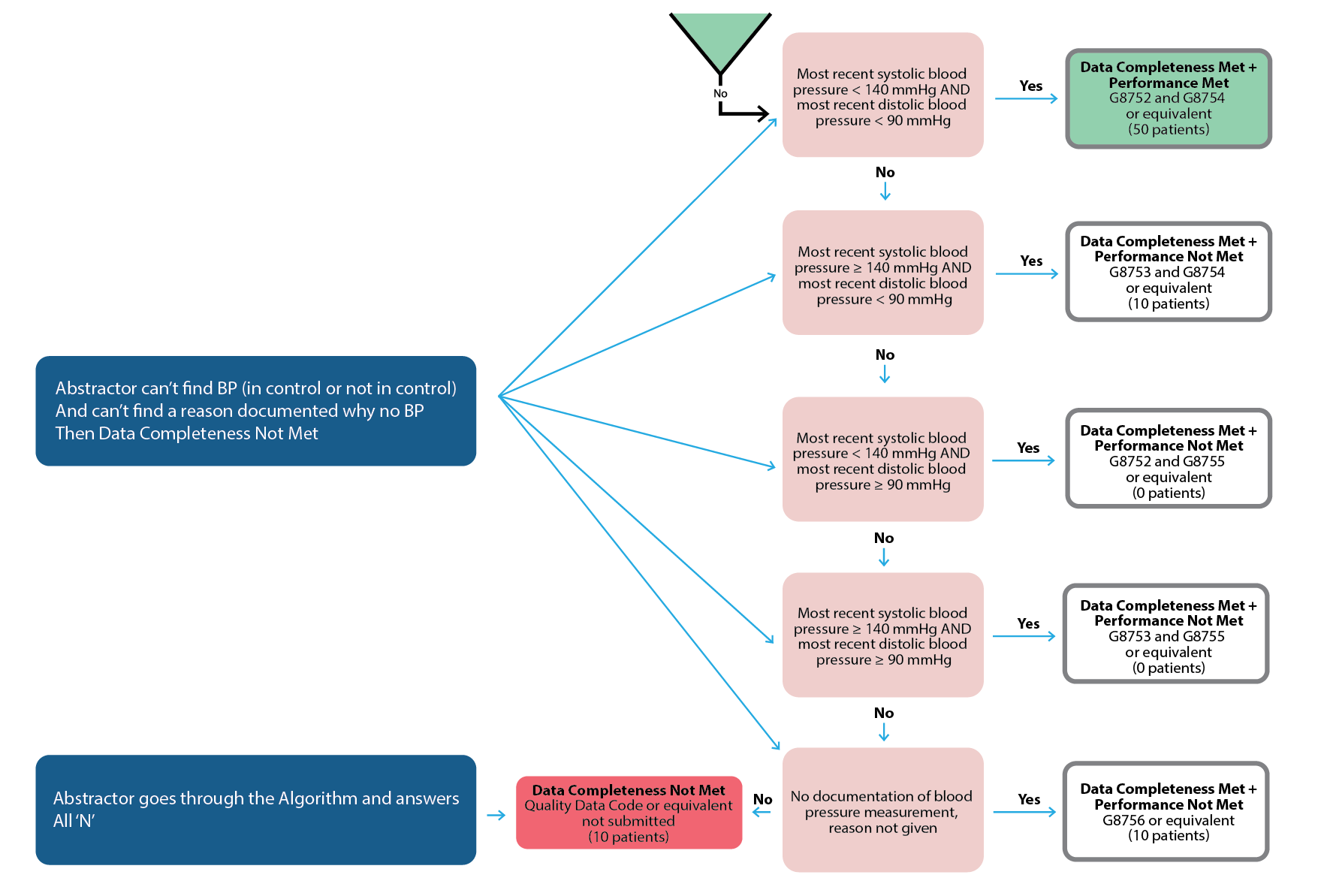
When is the data completeness threshold applicable?
It’s an unlikely scenario. But in some cases, an abstractor can't find the documentation that’s required by the measure. In this red scenario below, an abstractor answers “no” to algorithm questions for more than 30% of cases.
How to Get Started With eCQM/CQM Reporting
ACOs must learn to juggle multiple, disparate EHRs and data collection methodologies. Developing a cohesive data aggregation system is going to be a major undertaking. Your senior leadership, quality management, and information technology teams need to start planning what that looks like for your ACO now.
The most important thing you can do right now is understand what your data landscape looks like. Here are a couple of questions you should know.
- Which practices are on which EMRs? Make a list.
- How many instances of each EMR vendor do you have?
- Do you have any practices still on paper charts? (<<If so, you cannot report PI to CMS, unless all clinicians in that practice aren’t eligible or they qualify as a Small Practice.)
- How many practices are on less common EMRs?
- Can every single practice generate a QRDA I file (<<Applicable for eCQMs. Especially focus on those practices with less common EMRs.)
- Do you capture CPT II (G codes) in a database for all practices? (<<Applicable for MIPS CQMs.)
This information will help you to choose whether you want to submit eCQMs or MIPS CQMs. It will also inform you as to whether or not you have to set up conversations with any practices not able to provide your group with what you need.
More Resources to Prepare Your ACO For What’s Next
At Medisolv, we offer so much more than quality software and start-to-finish submissions management. We’re the quality improvement partner committed to deciphering and anticipating CMS’s regulatory changes for you—so that you can keep your organization ahead of the curve.
Check out some of our additional resources now:
- Article: 2025 QPP Requirements
- On-Demand Webinar: Preparing your ACO for APP Reporting
Medisolv Can HelpAlong with award-winning software, each client receives a dedicated Clinical Quality Advisor that helps you with your technical and clinical needs. We consistently hear from our clients that the biggest differentiator between Medisolv and other vendors is the level of one-on-one support. Especially if you use an EHR vendor right now, you’ll notice a huge difference.
|


.png?width=352&name=2026%20Quality%20Reporting%20Deadlines%20Guide%20(1).png)

Comments