

The Joint Commission introduced a new perinatal eCQM last year—ePC-06 (Unexpected Complications in Term Newborns)—for accredited hospitals that deliver more than 300 babies a year. Kristen Beatson, RN, shares who should consider this measure and how to collect data for it.
The Joint Commission introduced a new perinatal eCQM last year: PC-06 (Unexpected Complications in Term Newborns).
The Joint Commission does not yet require hospitals to submit PC-06 for accreditation purposes. But given the rising concern over mother and baby care more hospitals may be submitting one or more PC measures to The Joint Commission in 2022. Given that possibility, we’re going to walk you through what you need to know to successfully implement PC-06 in your own quality department.
Four Reasons PC-06 is Complicated to Implement
PC-06, which measures the percent of full-term newborns with unexpected complications, is unexpectedly complicated to implement. But when you look under the hood, you’ll understand why.
- Constructing PC-06 requires you to collect and map huge numbers of data elements before you send it electronically to The Joint Commission. For example, PC-06 includes 34 of value sets, which are basically diagnoses, procedures and treatments for newborns. Each value set includes different codes that fall within a particular diagnosis, procedure or treatment. One value set, congenital malformations, has nearly 7,000 different codes alone. You must correctly map to each code and each data element in each value set to automatically pull that information into the numerator of your measure.
- Virtually every data element you need to collect and map to requires a date and time stamp. In maternity care, when things happen is important to know for safe and effective medical care. When did the mother’s blood pressure rise? When did the fetus’ heart rate slow? When did contractions start?
- Data could come from multiple IT systems. Complications could occur in lots of different places: the emergency room, during pre-admission, on the labor and delivery floor, in an operating room or in recovery. That means you must pull your data elements from different IT systems, not just the patient’s inpatient EHR, to capture what you need and reconcile any discrepancies in dates and times.
- Evaluating the numerator itself is complicated. The numerator is stratified. All data must be correctly dated and timed for each of the value sets in both strata: newborns with severe complications, based on three different criteria; and newborns with moderate complications, based on six different criteria. In addition, the measure is scored by proportion which is a new approach to calculating eCQM performance rates.
Implementing a new eCQM
When you begin the process of implementing a new eCQM it’s extremely important to have the correct people involved in the implementation process. This is a PC measure so it will help you if you get representatives from your OB unit who understand how the workflow goes and who understand the documentation process. Get their input as well as clinician input so that you implement this measure in a way that works for them.
2022 ORYX® Requirements
As a quick reminder, for your 2022 ORYX® eCQM requirements, you must select four of the 13 available eCQMs and submit three quarter’s worth of data.
Starting last year, TJC allowed hospitals to submit any or all of the required chart-abstracted Perinatal Care Measures (PC-01, PC-02, PC-05 and PC-06), as the eCQM version instead of four quarters of the corresponding chart-abstracted measure. So essentially, you could meet your eCQM and chart-abstracted requirements for TJC through only an eCQM submission.
List of available eCQM measures for 2022 reporting:
- ED-2 Admit Decision Time to ED Departure
- OPI-1 Safe Use of Opioids
- PC-01 Elective Delivery Available
- PC-02 Cesarean Birth
- PC-05 Exclusive Breast Milk Feeding
- PC-06 Unexpected Complications in Term Newborns
- PC-07 Severe Obstetric Complications
- STK-2 Discharged on Antithrombotic Therapy
- STK-3 Anticoagulation Therapy Available
- STK-5 Antithrombotic Therapy
- STK-6 Discharged on Statin Medication
- VTE-1 Venous Thromboembolism Prophylaxis
- VTE-2 ICU Venous Thromboembolism Prophylaxis
Understanding the ePC-06 Specification
When I read the specification, I always start with the rationale and guidance, and in this case, I think the rationale helps you to understand why you would want to implement this measure. It provides you with a good explanation that you can share with your team.
Here’s the specification. I suggest you follow along with the HTML version as you read.
We are going to start at the top of the spec sheet with the Rationale.
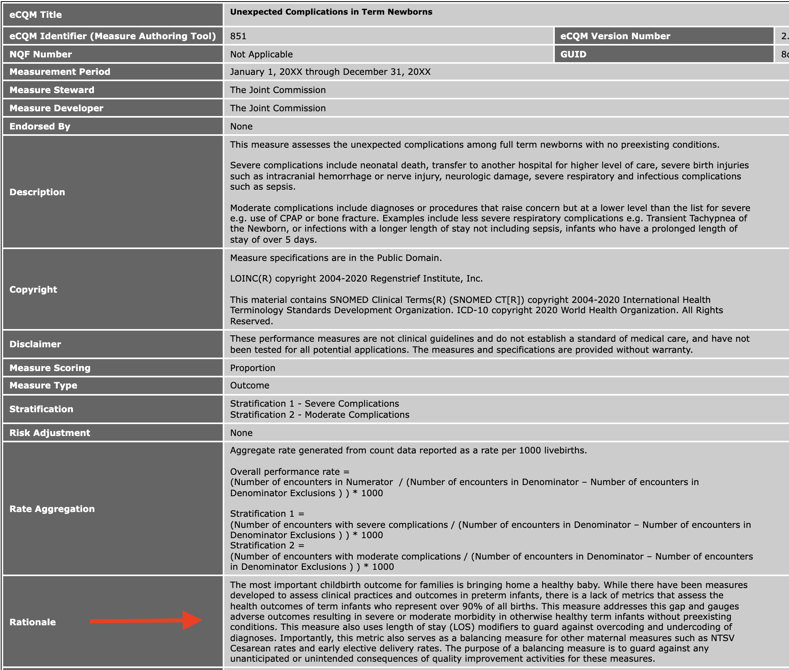
The Rationale in Layman's Terms
They are calling this measure a balancing measure for the other PC measures such as cesarean births and elective delivery rates. As we know can happen, sometimes by attempting to fix one problem, we cause unintentional problems elsewhere.
This measure was intended to guard against that by measuring the morbidity for otherwise healthy full-term babies.
Reading an eCQM specification
At the top of the specification are things like rationale and guidance, but it’s the bottom of the spec that’s important for you to dissect and understand. The bottom of the spec is the logic section which contains the Population Criteria, Definitions, Terminology and Data Criteria (QRD Data Elements). This can appear overwhelming and confusing at first but it’s quite logical if you follow along. And for anyone who is used to reading specs in the old language, remember that we moved over to the CQL language now which is different.
Understanding the eCQM Specification Logic
To understand the logic, you first read the population criteria statement(s). Then scroll down and find the definitions for all of the statements found in those population criteria groups.
For example, to understand who are defined in the “Initial Population” population criteria section, read the statement under “Initial Population.” In this case it says “PCNewborn."Single Live Term Newborn Encounter During Measurement Period."
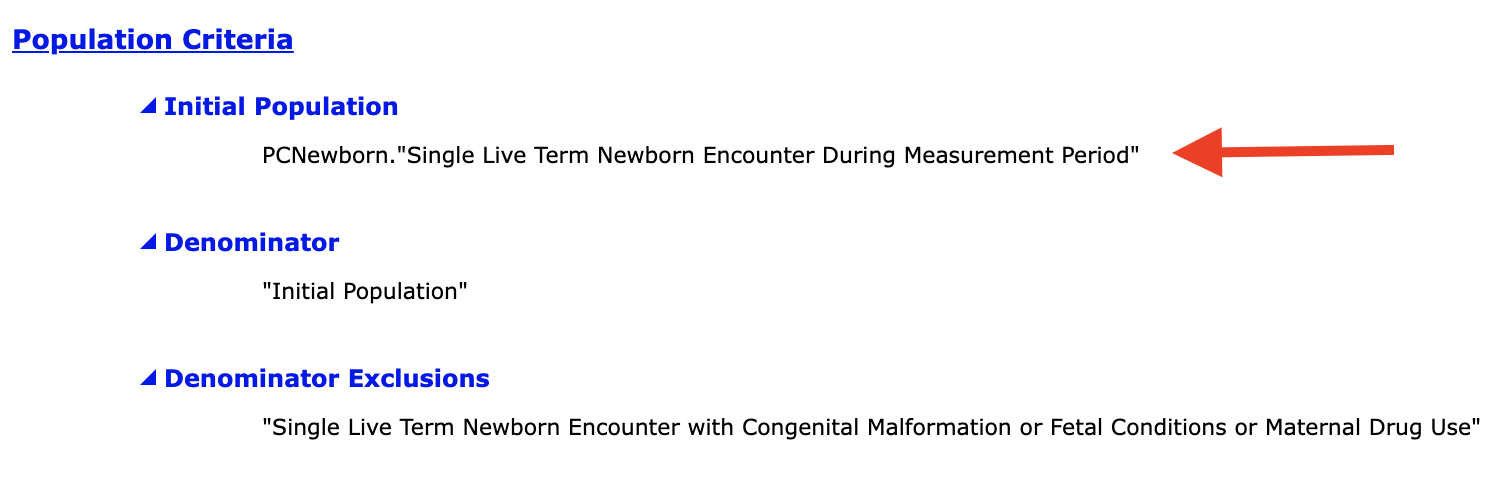
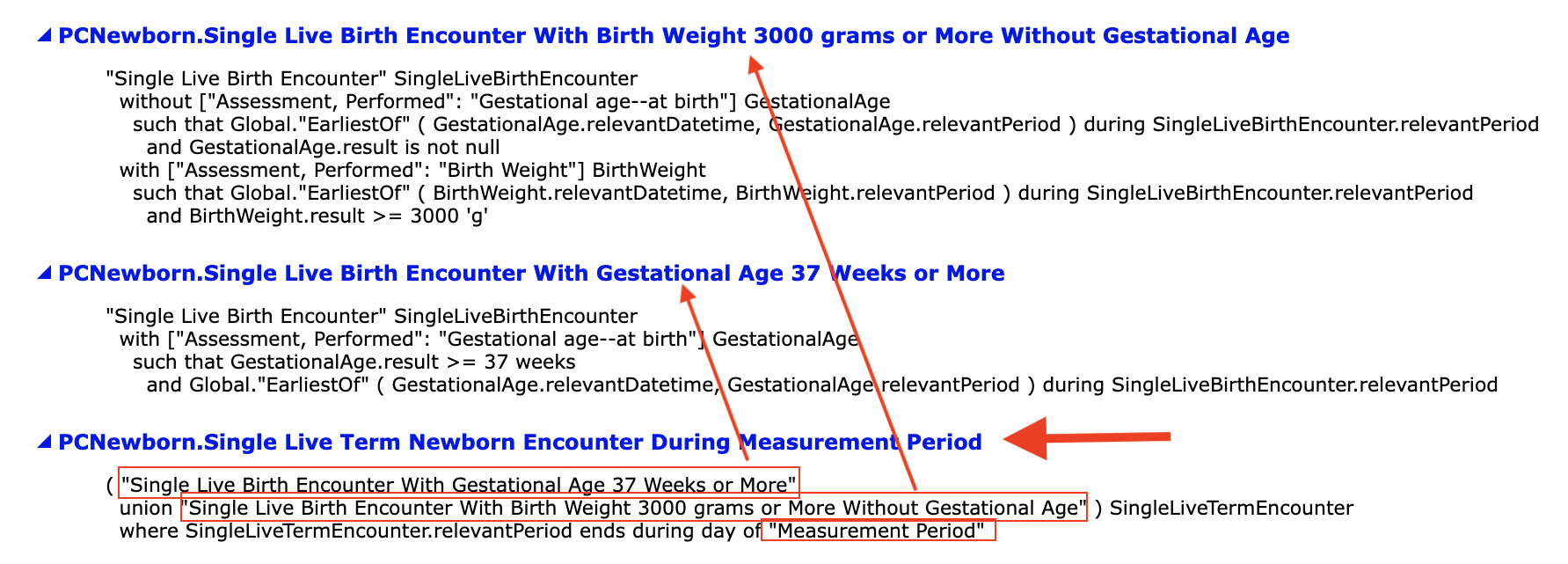
You then scroll down to the Definitions section and locate the definition for “PCNewborn."Single Live Term Newborn Encounter During Measurement Period." This definition contains other terms in quotes that have separate definitions that you must find and then read through.
Look at the picture below. In this definition we are reviewing, it is defined as “Single Live Birth Encounter with Gestational Age 37 Weeks or More” union “Single Live Birth Encounter with Birth Weight 3000 grams or More without Gestational Age.” Each of those statements in quotes has a corresponding definition (also pictured). You must then go read the definition for every single definition until you completely and fully understand what this measure is asking of you.
We’ve found this is the path most quality leaders take actually.

Do you know CMS calls this spec the human-readable version???
Mapping eCQMs Using the Data Elements
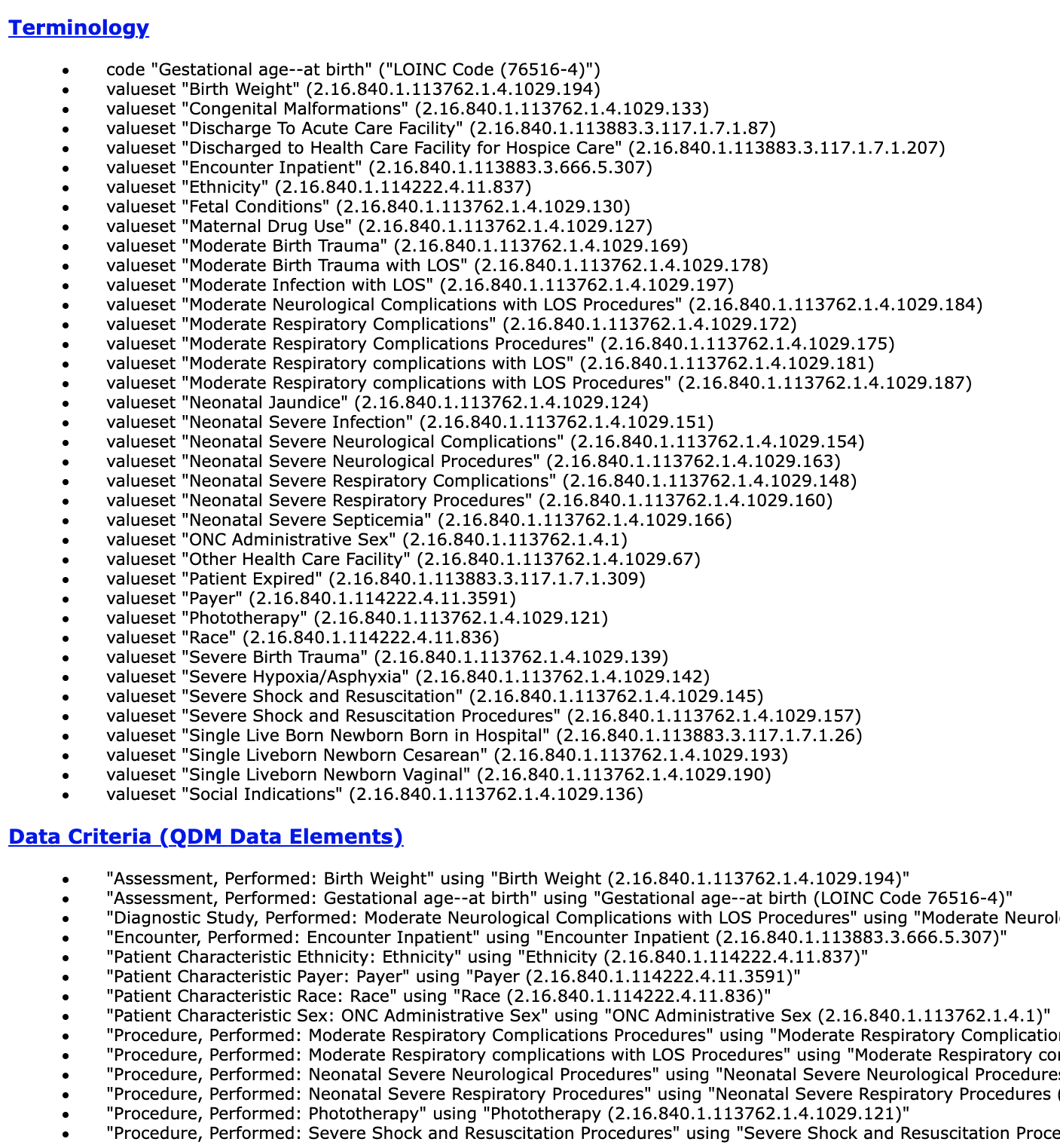
At the very bottom of the spec is the Data Criteria (QDM Data Elements) section which contains the value sets you’ll need to map in order to properly capture those data elements found in the definitions section. At the end of each bullet, you’ll see a long string of numbers. These are OID codes which are used to look up the value sets on the VSAC website. Those value sets provide you the codes you need to map in order to capture that particular data element. For Medisolv clients, you don’t have to go to VSAC, your Clinical Quality Advisor will provide them or you can look up those value sets right in the software.
A review of the population criteria for PC-06
You’re probably a little confused. Here, I’ve simplified the logic from what we looked at above and listed the populations with just the significant data elements that you need to consider as you are setting up the PC-06 measure.
The first thing to know is that this is an inverse measure. You want a low performance rate. You do not want babies in your numerator.
Let’s start with the Initial Patient Population which contains the first group of patients that qualify for the measure.
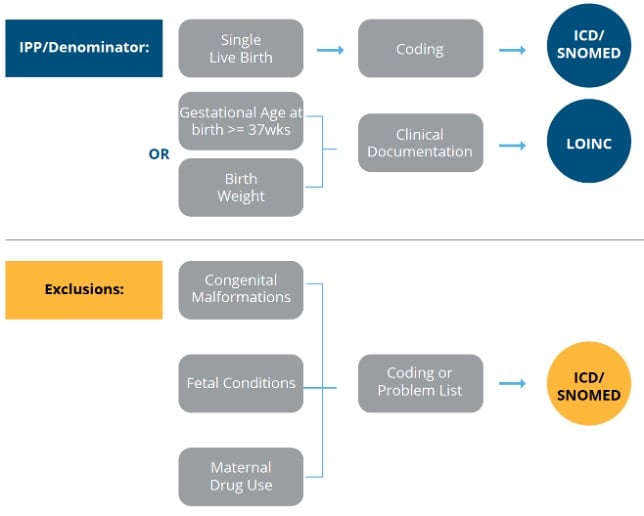
Initial Patient Population/Denominator
Layman’s description: To get into the Initial Patient Population (IPP) the baby must have a gestational age of greater than or equal to 37 weeks or no age documented. It has to have been a single live birth and they have to weigh greater than or equal to 3000 grams.
Simplified logic: Initial Population / Denominator
- Single Live Birth
- Gestational Age at birth >=37 weeks
or
- Single Live Birth
- Birth Weight >=3000 grams
- No Gestational Age documented during encounter
For this measure, the Initial Patient Population and Denominator are the same so once you’ve got this group of patients defined, we want to see if any of them will be moved into the Exclusion population.
Exclusions
Layman’s description: Once patients enter into the Denominator population, they may be put into the Exclusion population if they have congenital malformations, fetal conditions or if there is documented maternal drug use.
Simplified logic: Exclusions
- Congenital Malformations
- Fetal Conditions
- Maternal Drug Use
And finally of the remaining patients in the Denominator (who were not excluded) we consider whether they make it into the Numerator population. For this measure, there are actually two stratifications – one for severe complications and the other for moderate complications.
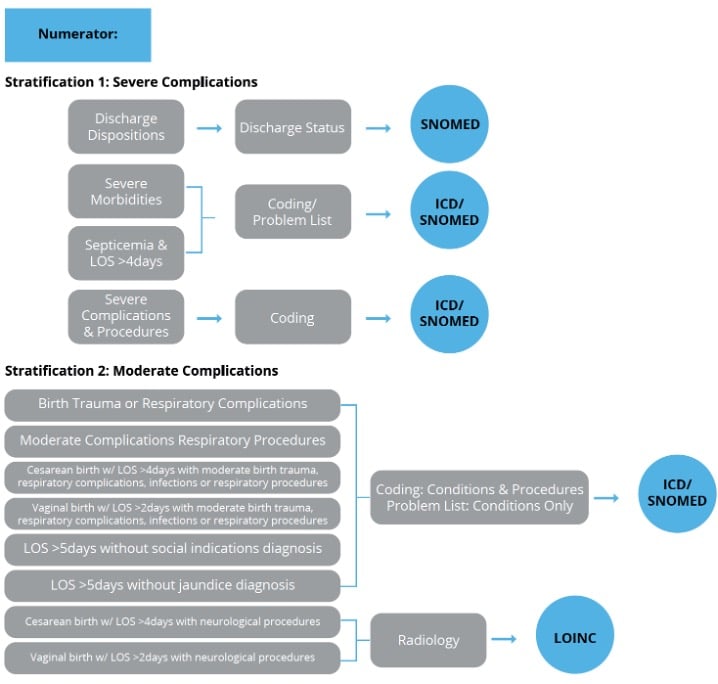
Numerator
Layman’s description: Anyone who made it into the Numerator who was not excluded and had one of these qualifying complications documented.
Simplified logic: Numerator
- Stratification 1 -Severe Complications
- Discharge Dispositions (Expired, To Acute Care Facility, Other Health Care Facility, Health Care Facility for Hospice)
- Severe Morbidities (6 value sets) or Severe Complications Procedures (3 value sets)
- Neonatal Severe Septicemia and length of stay > 4 days
- Stratification 2 -Moderate Complications
- Birth Trauma or Respiratory Complications (2 value sets)
- Moderate Complication Procedures (1 value set –Respiratory Procedures)
- Cesarean birth and length of stay > 4 days with moderate birth trauma, respiratory complications, infections, or neuro or resp procedures
- Vaginal birth and length of stay > 2 days with moderate birth trauma, respiratory complications, infections, or neuro or resp procedures
- Length of stay > 5 days without jaundice diagnosis
- Length of stay >5 days without social indications diagnosis
Your performance rate is then calculated using these populations. Remember, a lower number is better.
Setting up the PC-06 workflow
Once you’ve pulled apart the specification the next step is to do a current state analysis of where these items are being captured in your current EHR set up. I find that a workflow graphic like the one I’ve provided below is helpful as you do this process.
You’ll see (from left to right) I listed the different populations followed by the population criteria statement(s), then an educated guess for where that documentation may be found in your EHR and then the type of codes you’ll need to map to capture that element.
As you look at each population criteria statement fill in the information for your specific organization.
- Do you capture this information?
- If not, what is the best way to capture the information going forward?
- If so, where do you currently capture this information?
- Will you need to make any changes to documentation processes?
- Are you capturing it in multiple places?
- If so, which documentation will give you the best results that are within the timing restrictions?
Once Set Up Validate
Once you have the measure set up in your system you can begin the validation process. Initially this process may take some time as you will be trying to resolve technical errors and problems with workflows, but after the kinks are worked out you can begin the real work of quality improvement.
Here is a screenshot of one of our client’s rates. Note how the populations match against the review we just did above.
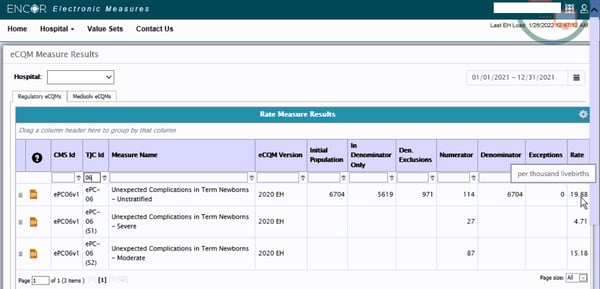
Implementing PC-06 is complicated, time-consuming and requires lengthy validation and testing. But making the effort will give you a more accurate calculation of your unexpected complication rate in full-term newborns. With that more accurate calculation, you can compare your performance with peer hospitals and drill down into your clinical protocols to improve outcomes for moms and their babies.
Don’t go it alone! Reach out to us today to talk about how we can help your team. Leave all this measure deciphering to us. We guide you as you set up the measure, troubleshoot technical errors and come up with strategies for improvement like clinician adherence. Request a demo of our ENCOR for Electronic Hospital Measures software today.

.jpg?width=352&name=The%20Top%205%20Challenges%20in%20Manual%20Clinical%20Data%20Abstraction%20(And%20How%20AI%20Can%20Fix%20Them).jpg)


Comments