

The Quality Payment Program has undergone some major changes over the last several years and CMS has signaled that they intend to further modify the program in the years to come. It's hard to keep all the requirements straight. In this article, we will cover the major themes that came out of the recent final ruling, review the base requirements for all participants and then review the individual requirements according to a clinician’s participation status.
Major Theme Changes
There are three major themes to the changes CMS unfolded as a part of the 2024 PFS Proposed Rule.
Theme 1: MSSP ACOs must start reporting using eCQMs, CQMs, or Medicare CQMs. CMS did not extend the deadline for transitioning away from CMS Web Interface measures. That means by 2025, everyone must report Quality measures as either eCQMs, CQMs, or Medicare CQMs.
Also see: eCQM vs CQM vs Web Interface: Understanding the Difference
Theme 2: Subgroup reporting by specialty type is here. CMS expanded their reporting framework called MIPS Value Pathways (MVPs). MVPs include measures that are for specific specialty groups (like rheumatologists). CMS added five more MVPs, bringing the total to 16 different MVPs a group could use to report in 2024. Full sub-group reporting is optional until 2026, when it becomes mandatory (if you choose to report this framework).
Also see: The 2024 MVP Reporting Bundle
Theme 3: The end of Traditional MIPS is hovering like a specter above us. CMS didn't commit to it, but they haven’t officially backed off their statement that says they will retire the Traditional MIPS reporting framework at the end of 2027, which would mean everyone must report under the MVP reporting framework (subgroup reporting by specialty type required) or be involved with an APM Entity (such as an ACO) and report through the APM Performance Pathway (APP) framework.
Let’s dive into the details.
Participation Eligibility
CMS puts Eligible Clinicians into one or more categories.
CMS puts Eligible Clinicians into one or more categories.
To find out your participation framework you must check your eligibility on the QPP website. Enter the provider NPI to determine eligibility.
- Not eligible
- You are not required to participate in MIPS but may have an option to opt-in to report. Your ability to opt-in depends upon how much you billed Medicare.
- MIPS Eligible Clinician Individual
- As an individual clinician you are required to report.
- MIPS Eligible Clinician Group
- As an eligible clinician, you are part of a group that is required to report. Groups are made up of clinicians who all bill with the same Tax ID (TIN).
Once you identify whether you are eligible to report as an individual or group, you may choose how to participate.
- Individual: Collect and submit your data as an individual.
- Group: Collect and submit data for all clinicians in the group.
- Subgroup: (MVP only) Collect and submit data for all clinicians in the subgroup.
- Virtual Group: (MIPS only) Collect and submit data for all clinicians in a CMS-approved virtual group. Virtual groups must be established before the start of the performance year.
- APM Entity: Collect and submit data for the clinicians identified as participating in the MIPS APM.
APM Entities will be referenced throughout.
APM stands for Alternative Payment Model. An APM Entity is responsible for reporting to this program on behalf of their participants.
Advanced APM Entity
An organization that takes on some form of financial risk. These organizations do not have to report to MIPS.
Other APM Entity
Those organizations not designated as advanced. ACOs make up a good portion of these types of organizations.
Reporting Frameworks
Understanding the Frameworks
Once you know your participation status, you will understand which framework you can use for submission. There are three QPP frameworks in 2024:
Traditional MIPS Framework
This is the usual MIPS framework made up of four categories and a composite score.
APM Performance Pathway (APP) Framework
The APP Framework is available to MIPS APM Entities and required for ACOs if they are part of MSSP.
MVP Framework
The MVP framework focuses on sub-group reporting by specialty type – applicable specialty measures designed for specialists. This reporting framework will eventually replace Traditional MIPS.
Here is a matrix of which framework you can report to, based on your status.
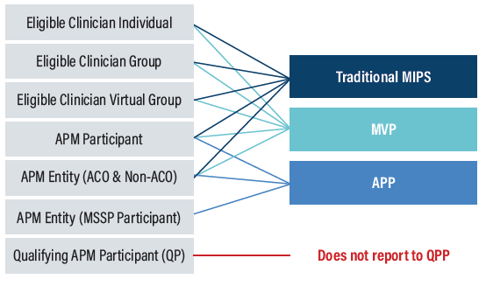
Each framework has slightly different requirements and different category weights.
Collection Types
Collection types are the way you report the data to CMS. You can think of them like measures. There are six collection types in 2024.
- eCQMs (Electronic Clinical Quality Measures)
- MIPS CQMs
- QCDR measures (Qualified Clinical Data Registry)
- Medicare Part B Claims measures
- CAHPS for MIPS survey
- CMS Web Interface measures (available for MSSP ACOs only)
As I mentioned before, CMS Web Interface is going away in 2025, so if this is the primary way you submitted your measures before, you need to figure out a new collection type soon.
Which collection type you can submit depends upon your participation status.
Now we are ready to review the requirements for each framework.
|
Learn how Medisolv helps hospitals navigate QPP changes in 2024 |
2024 Quality Requirements
2024 Promoting Interoperability Requirements
2024 Improvement Activities Requirements
2024 Cost Requirements
2024 Population Health Requirements
2024 Bonus Points
There are many opportunities to get bonus points within the MIPS program.
Improvement Bonus: Up To 10 Points
Clinicians will be rewarded if they demonstrate any improvement to their 2023 Quality score over the prior year (pending there is enough data for comparison). New Clinicians will be rewarded up to 1 additional point for improvement to their Cost performance scores.
Complex Patient Bonus: 5 Points
For clinicians who work with patients that have more complex cases, CMS will award up to 5 points to account for the additional complexity of treating their patient population.
Small Practice Bonus: 6 Points
An additional 6 bonus points will be added to the numerator of the Quality category for anyone qualifying as a small practice.
2024 Score Threshold Reimbursement
Applicable to MIPS and MVP Reporting Frameworks
To avoid a -9% penalty, you must score at least 75 points.
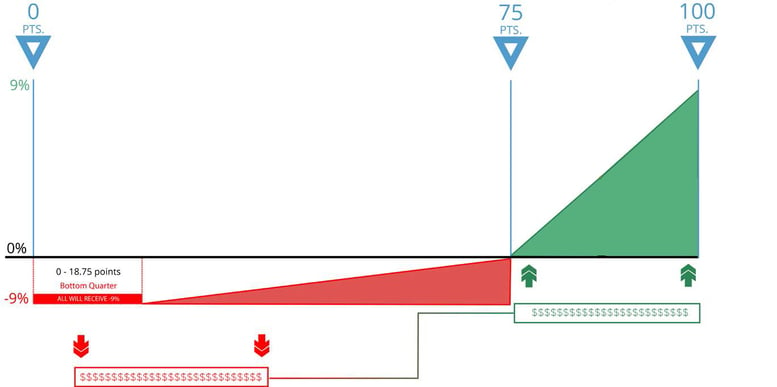
0-18.75 Points
If your score is between 0 and 18.75 points, you will lose -9% from your Medicare fee schedule (in red above).
18.76-74.99 Points
If your score is between 18.76 and 74.99 points, you will receive a reduction to your Medicare fee schedule between -8.99% and 0%
75 -100 Points
75 points is the performance threshold. CMS will take the funds of those who did not meet the threshold (in red) and distribute them among those who did meet the threshold (in green). Anyone whose MIPS score is between 75 and 100 points will receive some portion of those funds – up to a 9% increase to your Medicare fee schedule.
Note: There is no longer an Exceptional Performance bonus
APP Reporting Framework - MSSP ACOs
Shared Savings
To get the maximum shared savings for your ACO you must:
Report ALL measures in the APP measure set
AND
Achieve the Quality Performance Standard
CMS has implemented a sliding scale to give ACOs some percentage of the Shared Savings (not max) if they don’t meet the quality performance standards but do achieve a quality performance score equivalent to or higher than the 10th percentile of the performance benchmark on at least one of the four outcome measures.
Maximize Your Shared Savings
Quality Performance Standard
- Report eCQMs/CQMs
- Achieve a score = > 10th percentile on 1 outcome measure
- Achieve a score = > 40th percentile on at least 1 of the remaining measure
OR
Health Equity-Adjusted score of => 40th percentile across ALL quality performance scores
CMS will calculate 2024 and 2025 benchmarks for the Medicare CQMs based on performance period benchmarks. They will transition to historical benchmarks in 2026 and subsequent years.
This means that ACOs will not know the Medicare CQM benchmarks during the performance period.
CMS is NOT extending the eCQM/MIPS CQM reporting incentive to Medicare CQMs.
CMS finalized the use of historical data to establish the 40th percentile MIPS Quality performance category score used for the quality performance standard.
That means you would know what the Quality Performance Standard percentile is BEFORE the performance year starts.
40th Percentile MIPS Quality Performance Category Scores Used in the Calculation of the PY 2024 Historical MIPS Quality Performance Category Score
| Performance Year |
40th Percentile of the MIPS Quality Performance Category Score |
|
2020 |
75.59^ |
|
2021 |
77.83^ |
|
2022 |
77.73^ |
|
2023 |
Skipped due to 1-year lag |
|
2024 |
77.05 |
^ PY 2020 through PY 2022 40th percentile scores are based on performance period data
Important Dates
January 1, 2024
The start date to track 365 days of Quality and Cost category measures.
April 1, 2024
Registration opens for CMS Web Interface, CAHPS for MIPS Survey, and MVP selection.
July 4, 2024
The last day to start measures in the Promoting Interoperability category to meet the minimum of 180 continuous days.
October 2, 2024
The last day to start Improvement Activities to meet the minimum requirement of 90 continuous days.
November 30, 2024
Last day to register for an MVP.
March 31, 2025
The last day to submit all of your performance data.
Medisolv's QPP PackageMedisolv Can HelpThis is a big year for Quality. Medisolv can help you along the way. Along with award-winning software you receive a dedicated Medisolv Clinical Quality Advisor that helps you with all of your technical and clinical needs with no time restraints or extra costs.
|


.png?width=352&name=2026%20Quality%20Reporting%20Deadlines%20Guide%20(1).png)

Comments